
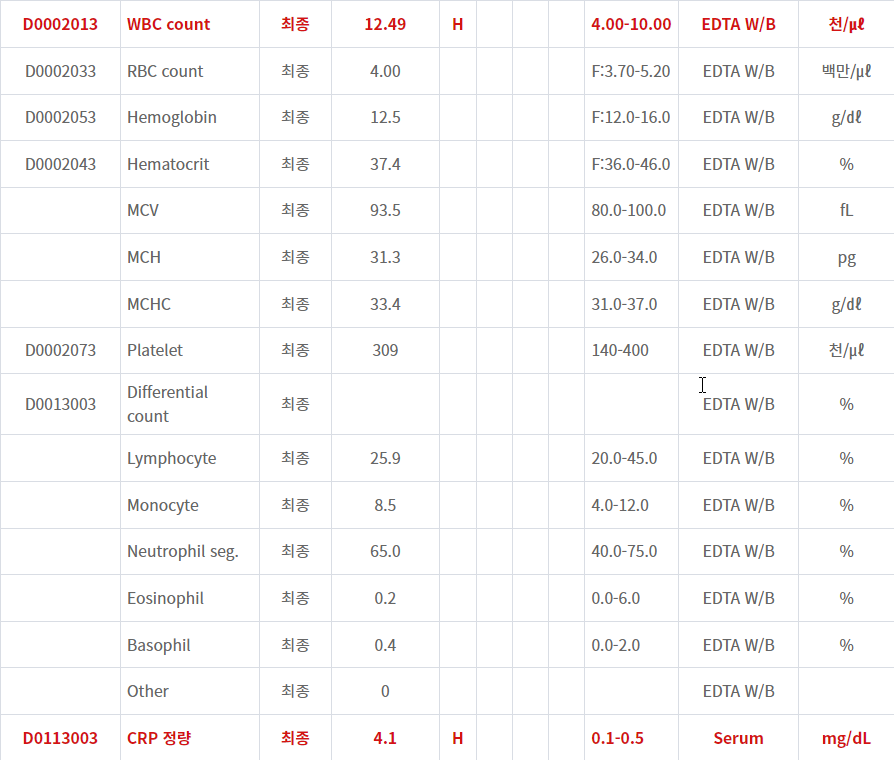
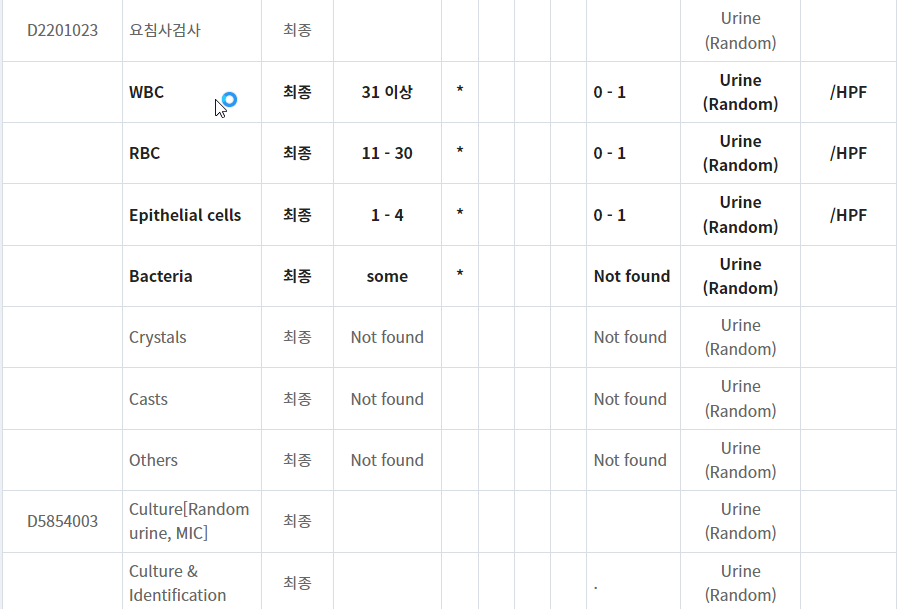
급성 신우신염에 대한 empirical antibiotics...
: 입원한 경우가 아닌 외래 환자에서 경험적 항생제 선택에 대한 내용입니다.
Fluoroquinolone에 대한 금기가 없고 이 약제에 대한 내성 위험이 낮은 경우 경구 fluoroquinolone을 경험적 항생제로 투약하며 용량은 ciprofloxacin 500 mg 하루 2회, 1000 mg 하루 1회, levofloxacin 750 mg 하루 1회 투약합니다. 치료 기간은 5-7입니다.
■ 퀴놀론 약제를 선택한 경우 치료 기간은 5-7일이다.
■ 퀴놀론을 사용하지 못하는 경우 아목시실린/클라블라네이트, 세프포독심, 세프디니르, 세파드록실을 선택할 수 있으며 치료 기간은 7-10일로 더 길다.
■ 세프트리악손, 어타페넴, 겐타마이신, 토브라마이신은 경구 약제 투약 이전에 1회로 외래에서 투약할 수 있고 ceftriaxone > ertapenem > gentamicin, tobramycin로 선택 순서를 갖는다.
■ 중증도에 따라 치료 기간을 길어질 수 있다.
Empiric antimicrobial agent selection for acute complicated urinary tract infection
|
Patient population
|
Risk for MDR?*
|
Empiric regimens
|
Comments
|
|
Outpatients
|
No, and no concerns with fluoroquinolones (eg, at low risk for adverse effects)
|
|
|
|
No, but with concerns with fluoroquinolones (eg, at risk for adverse effects)
|
|
|
|
|
Yes
|
|
|
* Risk factors for MDR gram-negative UTIs include any one of the following in the prior three months:
- An MDR, gram-negative urinary isolate, including a fluoroquinolone-resistant Pseudomonas urinary isolate
- Inpatient stay at a health care facility (eg, hospital, nursing home, long-term acute care facility)
- Use of a fluoroquinolone, TMP-SMX, or broad-spectrum beta-lactam (eg, third- or later-generation cephalosporin)
- Travel to parts of the world with high rates of MDR organisms
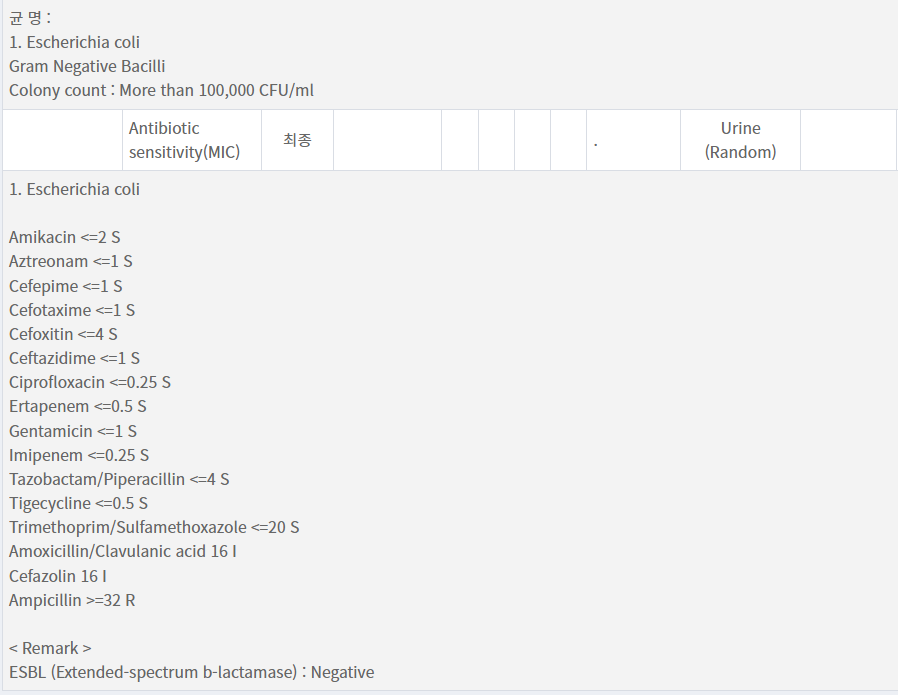
Empirical antibiotics : ciprofloxacin 500 mg bid for 10 days...경과가 좋으면 7일까지만 처방하자
'감염내과 > 요로감염' 카테고리의 다른 글
| Methenamine Hippurate는 여성에서 재발성 요로감염을 예방한다. (0) | 2023.01.24 |
|---|---|
| 급성 신우신염, 항생제 (0) | 2023.01.05 |
| ESBL 양성 대장균, 급성 방광염, 경구 항생제 선택 (0) | 2022.04.18 |
| 임신부 무증상 세균뇨, 추적검사와 치료는 어떻게 하나요? (0) | 2021.05.29 |
| 임신부 무증상 세균뇨, 왜 치료해야 하나요? 그리고 항생제 (0) | 2021.05.29 |



