
ASCVD, 당뇨병, 만성콩팥병증, 가족성 고콜레스테롤혈증이 없는 사람
→ 국가에 따른 위험군, 나이, 혈압, 성별, non-HDL-C에 따른 위험 구분




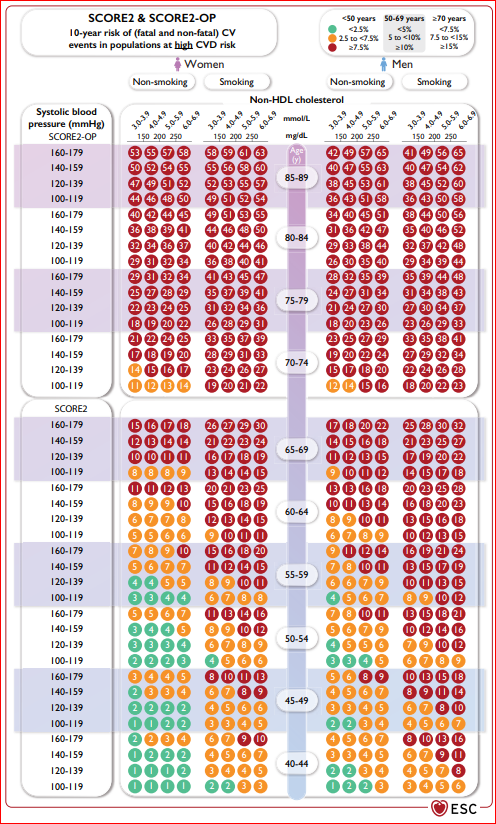

Figure 3 Systematic Coronary Risk Estimation 2 and Systematic Coronary Risk Estimation 2-Older Persons risk charts for fatal and non-fatal (myocardial infarction, stroke) cardiovascular disease.
SCORE2 = Systematic Coronary Risk Estimation 2; SCORE2-OP = Systematic
Coronary Risk Estimation 2-Older Persons; TFYR = The Former Yugoslav Republic; UK = United Kingdom. For apparently healthy people aged 40-69 years, the SCORE2 algorithm is used to estimate 10-year risk of fatal and non-fatal (myocardial infarction, stroke) CVD. For apparently healthy people ≥70 years of age, the SCORE2-OP is used.
- Low risk countries : Belgium, Denmark, France, Israel, Luxembourg, Norway, Spain, Switzerland, the Netherlands, and the UK.
- Moderate risk countries : Austria, Cyprus, Finland, Germany, Greece, Iceland, Ireland, Italy, Malta, Portugal, San Marino, Slovenia, and Sweden.
- High risk countries : Albania, Bosnia and Herzegovina, Croatia, Czech Republic, Estonia, Hungary, Kazakhstan, Poland, Slovakia, and Turkey.
- Very-high-risk countries : Algeria, Armenia, Azerbaijan, Belarus, Bulgaria, Egypt, Georgia, Kyrgyzstan, Latvia, Lebanon, Libya, Lithuania, Montenegro, Morocco, Republic of Moldova, Romania, Russian Federation, Serbia, Syria, TFYR (Macedonia), Tunisia, Ukraine, and Uzbekistan.
Meta-analysis of clinical trials has indicated that the relative reduction in CVD risk is proportional to the absolute reduction of LDL-C, irrespective of the drug(s) used to achieve such change, with no evidence of a lower limit for LDL-C values or ‘J-curve’ effect. LDL-C를 낮추는 절대적인 이득은 ASCVD의 절대적 위험과 LDL-C의 절대적 감소에 달려 있다. ASCVD가 높을수록 이득이 높고 LDL-C 감소가 클수록 이득이 높다. The absolute benefit of lowering LDL-C depends on the absolute risk of ASCVD and the absolute reduction in LDL-C, so even a small absolute reduction in LDL-C may translate to significant absolute risk reduction in a high- or very-high-risk patient. A recent LDL-C target-driven RCT in patients after ischaemic stroke or transient ischaemic attack (TIA) demonstrated a target LDL-C level of <1.8 mmol/L (70 mg/dL) with the use of statin and, if required, ezetimibe, was associated with a lower CVD risk than those who had a target range of 2.32.8 mmol/L (90-110 mg/dL)
공복 (fasting) 또는 non-fasting 측정
Lipid parameters의 non-fasting 측정이 일반 인구 스크리닝 검사에서 권고된다. Fasting sample과 같은 예후적 가치를 지닌다. 대사증후군, 당뇨병, 고중성지방혈증에서 c-LDL-C 해석 시 주의를 요한다.
■ LDL-C을 직접 측정할 수 있지만 다음과 같이 대부분 계산한다.

이러한 계산은 중성지방이 400 미만일 때 타당하고 LDL-C이 50까지 매우 낮으면 정밀하지 않다. LDL-C이 매우 낮거나 고중성지방혈증이 있는 경우는 다른 공식을 사용하던지 LDL-C을 직접 측정한다.
■ Apilipoprotein B는 특히 고중성지방혈증 환자에서 atherogenic lipid particles 총 농도의 직접적 추정치를 나타낸다. 그러나 apolipoprotein B가 제공하는 정보는 보통 c-LDL-C과 유사하다.

■ Non-HDL 콜레스테롤
총 콜레스테롤에서 HDL 콜레스테롤을 빼면 되는데 LDL-C에서 언급되었던 고중성지방혈증 400 미만을 요구하지 않는다. 이것은 또한 공복이지 않아도 정확하고 당뇨병 환자에서도 그렇다. We suggest it as a reasonable alternative treatment goal for all patients, particularly for those with hypertriglyceridaemia or DM.
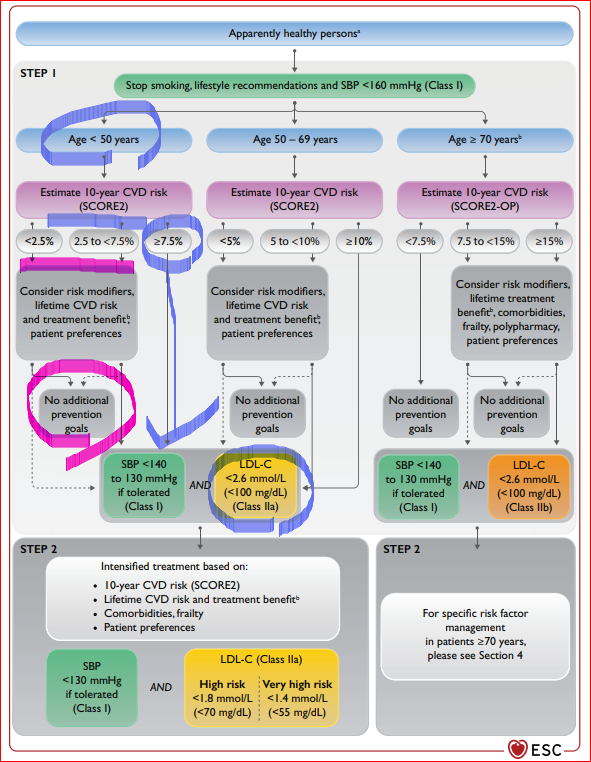
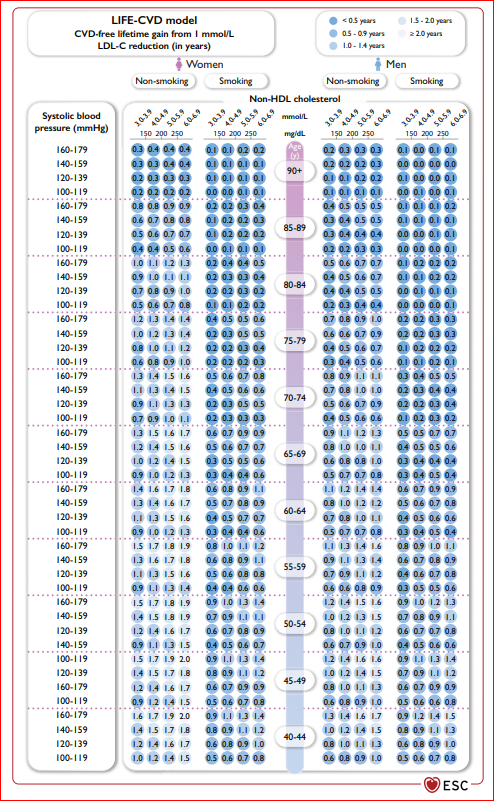
■ 건강한 성인에서 LDL-C 감소의 평생 치료 이득은 환자-의사간 치료 시작 상담에 도움이 된다. 다음은 low-modrate countries의 건강한 성인에서 LDL-C을 40 감소시켰을 때 CVD에서 자유로울 수 있는 평균 기간 (year) 이득이다. ■ 이 가이드라인은 stepwise approach를 권고하며 step2에서 치료 강화 수준은 이전 2016 ESC prevention Guideline에서 가장 낮은 LDL-C 목표 수치인 70 mg/dL보다 더 낮다. 이번에는 ASCVD가 있거나 very high risk인 경우 < 55 mg/dL가 목표이다. ■ 최근 2년 이내에 ASCVD를 경험하였다면 40 mg/dL까지 낮추는 것도 고려될 수 있다. 치료 이득 차이는 남녀 사이, 젊은/고령 사이, 당뇨 유무에 따라 달라지지 않는다.
REF.
1. European Heart Journal (2021) 42, 3227-3337, 2021 ESC Guidelines on cardiovascular disease prevention in clinical practice
2. 2022 송파구의사회 추계 온라인 학술대회
'내분비내과 > 이상지질혈증' 카테고리의 다른 글
| 스타틴이 총 사망률에 미치는 영향 <대한내과학회지: 제 98 권 제 1 호 2023> (1) | 2023.02.03 |
|---|---|
| 에볼로쿠맙 2023.01 급여기준과 심혈관질환 2차 예방에 대한 장기적 효과 (1) | 2023.01.23 |
| 스타틴 복용 후 콜레스테롤 수치 감소로 약제 중단 [이상지질혈증, 고지혈증, 고콜레스테롤혈증] (0) | 2022.11.20 |
| 고중성지방혈증에서 LDL-C 평가와 치료를 먼저할 것 (0) | 2022.11.09 |
| 고지혈증약, 스타틴 관련 근육 증상 시 스타틴 교체 (0) | 2022.06.23 |



