|
Incidentalomas 부신우연종은 30세 미만에서는 일반적이지 않고 나이가 증가하면서 빈도가 증가합니다. Incidentally discovered adrenal masses have become a common clinical problem. An adrenal mass is uncovered in up to 4% of patients imaged for nonadrenal disease. Incidentalomas are uncommon in patients younger than 30 years of age but increase in frequency with age; they occur more frequent in females, most commonly in the sixth and seventh decades. 임상적으로 2가지 문제가 중요합니다. 첫째는 기능을 하는가 (호르몬 분비)이고 두번째는 악성인가 여부입니다. 분명한 임상 특징이 있는 호르몬 분비 종양과 악성종양은 모든 부신우연종의 약 4%정도입니다. Clinically, two issues arise: whether the lesion is functional (i.e., secreting hormones) and whether it is malignant. Most incidentalomas are adrenocortical adenomas, but occasionally they represent myelolipomas, hamartomas, or granulomatous infiltrations of the adrenal gland and result in a characteristic CT/MRI appearance . Functioning tumors with a clear clinical phenotype (pheochromocytomas and those secreting cortisol, aldosterone, or sex steroids) and carcinomas account for around 4% of all incidentalomas. 비정상 호르몬을 분비하지만 명백한 임상 발현이 없는 경우도 있습니다. 대표적인 예가 subclinical Cushing syndrome입니다. In addition, it is established that some incidentalomas cause abnormal hormone secretion without obvious clinical manifestations of a hormone excess state. The best example is so-called subclinical Cushing syndrome, which occurs in up to 20% to 30% of all patients with adrenocortical incidentalomas. There is debate as to the best means to biochemically define this phenomenon, but serum cortisol after dexamethasone testing has the widest acceptance, although cutoff values vary. The European Society of Endocrinology and European Network for the Study of Adrenal Tumors (ENSAT) have published guidelines for diagnosis and management. When there is evidence of low-grade excess biochemical hypercortisolism, there is an associated increase in the prevalence of diabetes, obesity, hypertension, new cardiovascular events, osteoporosis, and fatality. However, no prospective study has proven that the adrenal adenoma is the cause of the observed complications, as these are highly prevalent in the population at this age. Intervention by adrenalectomy has shown some benefit, particularly lower blood pressure, but the studies performed have been largely retrospective and highly selected, and hence the approach to each patient needs individualization with most being observed in current clinical practice. 모든 발견된 부신우연종 환자들에서 적절한 내분비 스크리닝 검사를 시행해야 합니다. 24-hour urinary metanephrine collection, measurement of plasma metanephrines, an overnight dexamethasone suppression test, 그리고 고혈압 환자에서 measurement of plasma renin and aldosterone입니다. DHEAS는 adrenal androgen secretion의 marker로서 측정되어야 합니다. Adenoma에서 분비된 autonomous cortisol secretion로 인하여 ACTH 농도가 억제된 환자에서는 DHEAS 수치가 낮습니다. High levels of 17OHP after ACTH stimulation tests은 21-hydroxylase의 부분적 결함을 시사합니다. 이것은 양측성인 경우에 측정되어야 합니다. As a result, all patients with incidentally discovered adrenal masses should undergo appropriate endocrine screening tests. This testing should comprise 24-hour urinary metanephrine collection or measurement of plasma metanephrines, an overnight dexamethasone suppression test, and for those with hypertension, measurement of plasma renin and aldosterone. DHEAS should be measured as a marker of adrenal androgen secretion. Low levels may occur in patients with suppressed ACTH concentrations due to autonomous cortisol secretion from the adenoma. Some studies have also documented high levels of 17OHP after ACTH stimulation tests, suggesting partial defects in 21-hydroxylase in some tumors, and this should be measured in cases of bilateral disease. 부신이 아닌 다른 곳에서 암이 있었던 환자에서는 명백히 부신의 악성 가능성이 높습니다. The possibility of malignancy should be considered in each case. In patients with a known extra-adrenal primary tumor, the incidence of malignancy is obviously much higher; for example, up to 20% of patients with lung cancer have adrenal metastases on CT scanning. In those with no evidence of malignancy, adrenal carcinoma is rare. 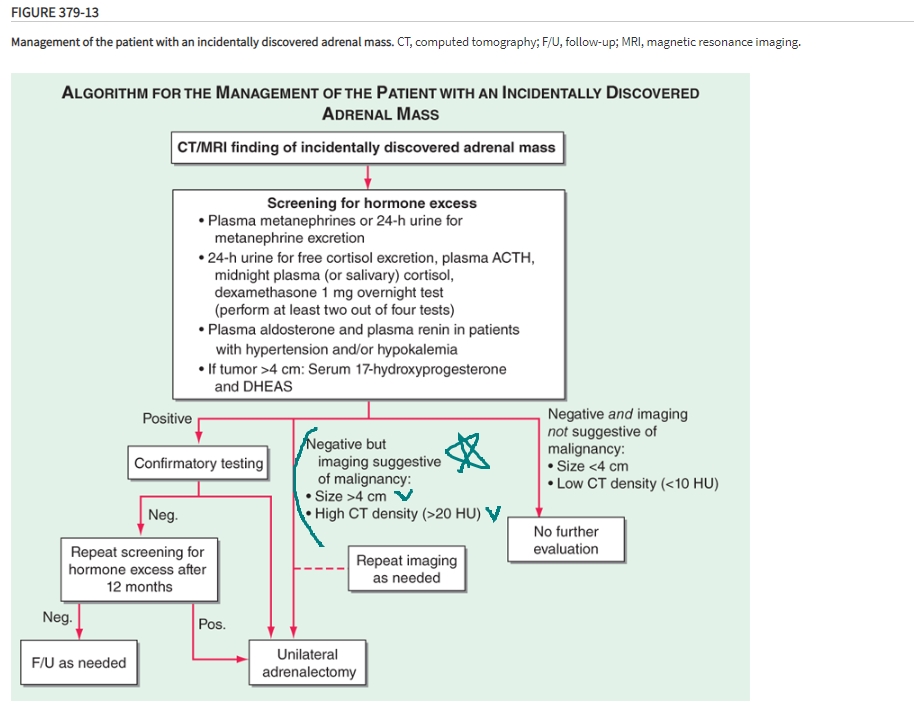 해리슨 20판 표에서도 언급된 악성을 시사하는 2가지 특징은 ① 크기와 ② HU 입니다.
 Distribution of diagnosis of adrenal incidentalomas. (A) Data from eight studies with histologically determined diagnoses ( n = 103) relating to tumor size. (B) Distribution of 380 incidental adrenal masses by histologic diagnosis. From Mansmann G, Lau L, Balk E, et al. The clinically inapparent adrenal mass: update in diagnosis and management. Endocr Rev. 2004;25:309–340. REF. 1. Williams Textbook of Endocrinology, 14th edition 2. Harrison's Internal Medicine, 20th edition 
|



