Ischemic stroke의 annual rate가 1.7% 이상은 되어야 와파린 사용에 이득. CHADS2 score (≥2)

Circulation: Cardiovascular Quality and Outcomes. 2011;4:14–21
Figure 1. One-way sensitivity analysis: Annual rate of ischemic stroke. Quality-adjusted life expectancy for each of the 3 strategies (warfarin, aspirin, and no antithrombotic therapy) is shown as a function of the annual rate of ischemic stroke ranging from 0 to 0.15 per year. There are 2 secondary horizontal axes showing the corresponding CHADS2 scores. The upper secondary axis uses the CHADS2 derivation cohort (see Appendix Table 2), whereas the lower axis maps the CHADS2 predictors to the annual stroke rate found in the more contemporary ATRIA cohort. The threshold lines divide the decision space into 3 regions. To the far left, at low rates of ischemic stroke (<0.2% per year), no antithrombotic therapy is best, whereas to the far right at stroke rates greater than 1.7% per year, anticoagulation with warfarin is best. There is a small region between these 2 thresholds in which aspirin use is preferred. Using more contemporary data for stroke risk (bottommost horizontal axis), anticoagulation is only preferred at a higher CHADS2 score (≥2), compared with stroke risk predicted by the CHADS2 derivation model (top secondary horizontal axis), for which warfarin is preferred even with a CHADS2 score less than 0.
Ischemic stroke의 annual rate가 0.9% 이상은 되어야 NOAC 사용에 이득. CHADS2 score of ≥1

Circulation: Cardiovascular Quality and Outcomes. 2011;4:14–21
Figure 2. One-way sensitivity analysis: Annual rate of ischemic stroke with addition of anticoagulation with a new, “safer” anticoagulant. The axes are the same as in Figure 1. With the addition of a new, “safer” agent as another option for anticoagulation, the “tipping point” above which the risk and outcomes of ischemic stroke outweigh the risk and outcomes of major hemorrhage shifts to the left. Anticoagulation with the new drug is preferred at annual stroke rates above 0.9% per year (CHADS2 score <0 in the derivation model; and CHADS2 score of ≥1 using the ATRIA data).
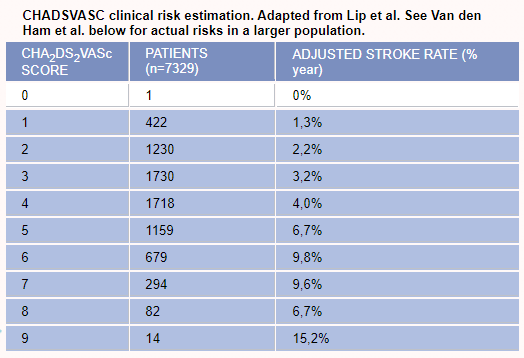
CHA2DS2-VASc scores가 1점 올라갈 때마다 adjusted ischemic stroke rate는 1.3%, 2.2%, 3.2%, 4% ~로 올라갑니다.
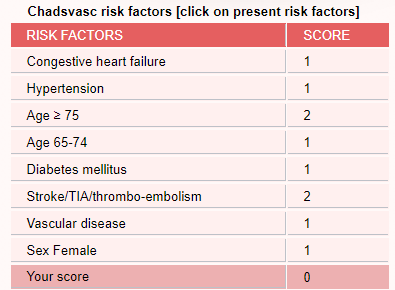
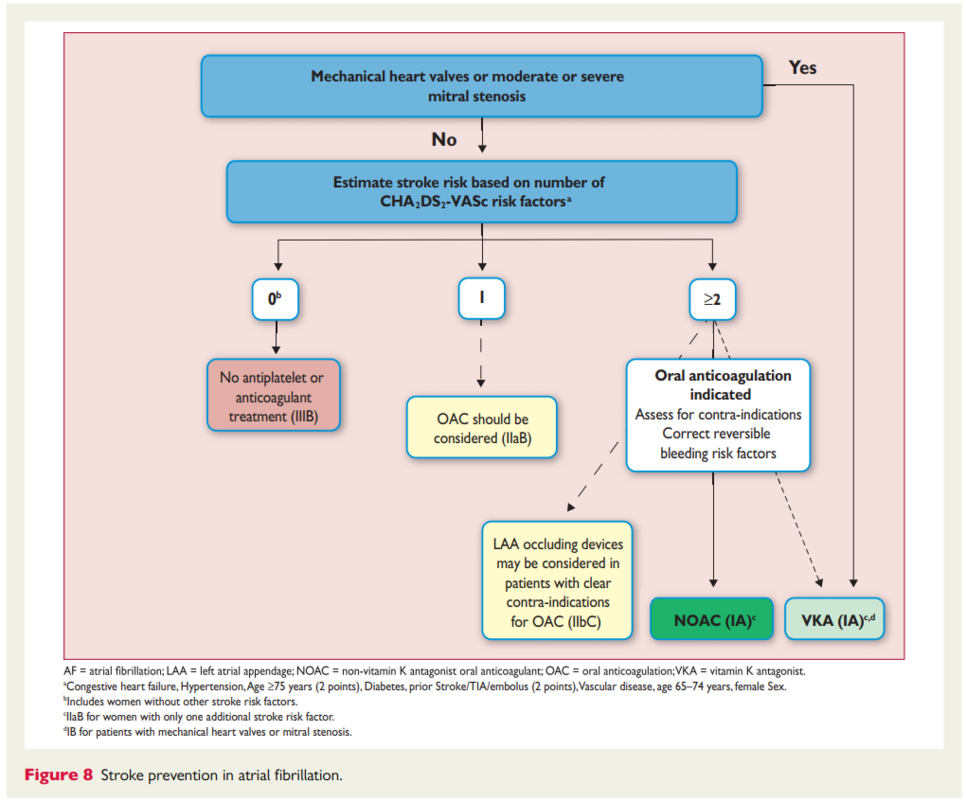
CHA2DS2-VASc scores 2점은 권고, 1점은 고려
국내 보험은 2점 이상에서 인정
항혈소판제는 뇌졸중 위험과 과련 없이 권고되지 않음

REF. Circulation: Cardiovascular Quality and Outcomes. 2011;4:14–21
ESC Guidelines AF 2016



