● 고혈압 기준이 되는 혈압은 수축기 130 mmHg 또는 이완기 80 mmHg 이상이다. 이 권고는 American College of Cardiology/American Heart Association 권고와 일치한다.
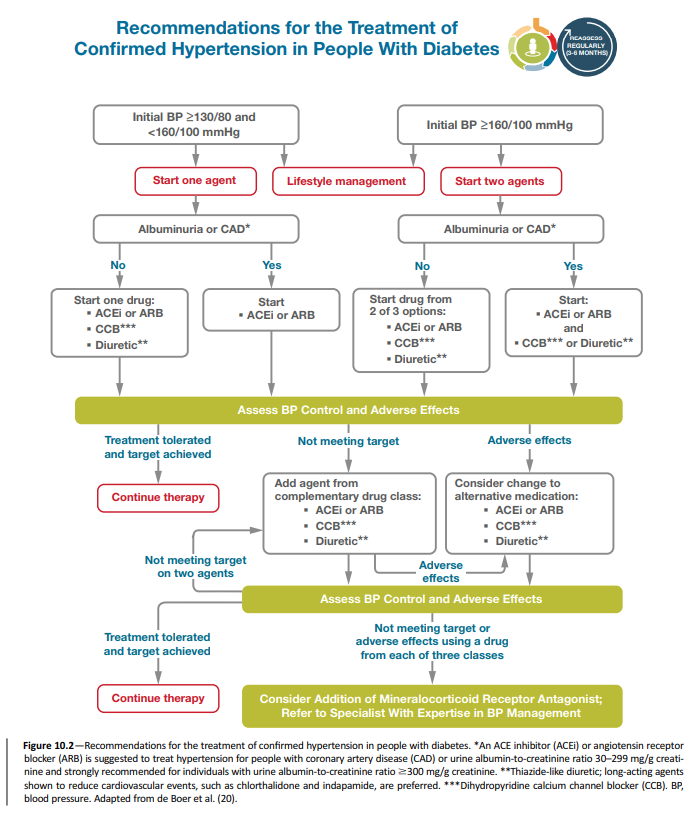
● 당뇨병과 고혈압이 있는 경우 약제 시작은 ≥130/80 mmHg이며 목표 혈압은 <130/80 mmHg이다. 이 권고사항을 지지하는 증거에 대한 논의는 광범위하게 개정되었다. 게다가 최근 보고된 STEP trial의 결과가 추가되었다.
● 권고되는 약물은 다음과 같다.
● 당뇨병과 만성 고혈압이 있는 임신부에서 약물 개시 또는 치료 적정의 목표 혈압은 140/90 mmHg이다. 목표 혈압은 110–135/85 mmHg이다.
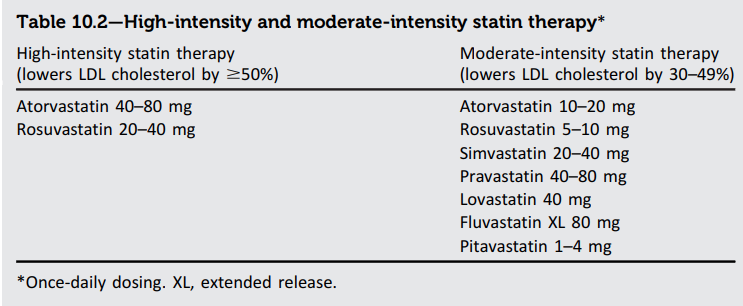
일차 예방 : 스타틴
● ASCVD가 없는 40–75세 당뇨병 환자에게 생활습관개선에 더하여 중강도 스타틴 치료를 시작한다.
● 1개 이상의 ASCVD 위험인자를 가지고 있는 40–75세 당뇨병 환자에게 기저 수치보다 LDL cholesterol ≥50% 감소시키고 LDL cholesterol 목표 <70 mg/dL에 도달하기 위해 고강도 스타틴 사용을 권고한다.
● Multiple ASCVD 위험 인자를 가고 있는 40–75세 당뇨병 환자에서 LDL cholesterol ≥70 mg/dL인 경우 복용 가능한 최대 스타틴에 더하여 ezetimibe 또는 PCSK9 inhibitor를 추가하는 것이 합리적일 수 있다.
● 이미 스타틴을 복용 중인 >75세인 당뇨병 성인에서 스타틴 치료를 지속하는 것이 합리적이다. 스타틴을 복용 중이지 않은 당뇨병 성인에서 잠재적 이득과 위험에 대한 논의 후 중강도 스타틴 치료를 시작하는 것이 합리적일 수 있다.
● 20-39세 당뇨병 환자에서는 추가적 ASCVD 위험 요인이 있는 경우 생활 습관에 더하여 스타틴 치료를 개시하는 것이 합리적일 수 있다.
● 임신 시 스타틴은 금기이다.
이차 예방 : 스타틴
● 당뇨병이 있는 모든 연령에서 ASCVD가 있는 경우 생활습관에 더하여 고강도 스타틴을 사용해야 한다.
● 이 경우에 치료 목표는 LDL cholesterol reduction of ≥50% from baseline and an LDL cholesterol goal of <55 mg/dL이다. 만일 목표에 도달하지 못하면 복용 가능한 최대 스타틴에 더하여 ezetimibe 또는 PCSK9 inhibitor가 권고된다.
Fibrate and niacin
● 공복 중성지방이 ≥500 mg/dL인 경우 고중성지방혈증의 이차 원인에 대한 평가를 하고 췌장염 위험 예방을 위해 약물 치료를 고려한다.
● 공복 또는 비공복 중성지방이 175–499 mg/dL인 경우 생활 요인 (비만, 대사증후군), 이차적 요인 (당뇨병, 만성간질환, 만성콩팥질환, 신증후군, 갑상선기능저하증), 고중성지방혈증을 일으키는 약물을 평가하고 치료해야 한다.
● ASCVD 또는 다른 심혈관 위험 인자가 있는 성인이 스타틴을 복용하면서 LDL 수치는 유지되고 있으나 중성지방이 상승되어 있는 경우 (135–499 mg/dL) icosapent ethyl 추가가 심혈관 위험 감소를 위해 고려될 수 있다.
● 스타틴과 fibrate를 병합하는 것은 ASCVD 결과 개선을 보여 주지 못했으므로 일반적으로 권고되지 않는다.
● 스타틴과 니아신을 병합하는 것은 단독 스타틴 치료에 더하여 추가적인 심혈관 이득 제공을 보여 주지 못했고 추가적 이상 반응에 더하여 뇌졸중 위험을 증가시킬 수 있어서 일반적으로 권고되지 않는다.
- 10.1 Blood pressure should be measured at every routine clinical visit. When possible, individuals found to have elevated blood pressure (systolic blood pressure 120–129 mmHg and diastolic <80 mmHg) should have blood pressure confirmed using multiple readings, including measurements on a separate day, to diagnose hypertension. A Hypertension is defined as a systolic blood pressure ≥130 mmHg or a diastolic blood pressure ≥80 mmHg based on an average of ≥2 measurements obtained on ≥2 occasions. A Individuals with blood pressure ≥180/110 mmHg and cardiovascular disease could be diagnosed with hypertension at a single visit. E
- 10.4 People with diabetes and hypertension qualify for antihypertensive drug therapy when the blood pressure is persistently elevated ≥130/80 mmHg. The on-treatment target blood pressure goal is <130/80 mmHg, if it can be safely attained. B
- 10.5 In pregnant individuals with diabetes and chronic hypertension, a blood pressure threshold of 140/90 mmHg for initiation or titration of therapy is associated with better pregnancy outcomes than reserving treatment for severe hypertension, with no increase in risk of small-for-gestational age birth weight. A There are limited data on the optimal lower limit, but therapy should be lessened for blood pressure <90/60 mmHg. E A blood pressure target of 110–135/85 mmHg is suggested in the interest of reducing the risk for accelerated maternal hypertension.
- 10.18 For people with diabetes aged 40–75 years without atherosclerotic cardiovascular disease, use moderate-intensity statin therapy in addition to lifestyle therapy. A
- 10.19 For people with diabetes aged 20–39 years with additional atherosclerotic cardiovascular disease risk factors, it may be reasonable to initiate statin therapy in addition to lifestyle therapy. C
- 10.20 For people with diabetes aged 40–75 at higher cardiovascular risk, including those with one or more atherosclerotic cardiovascular disease risk factors, it is recommended to use high-intensity statin therapy to reduce LDL cholesterol by ≥50% of baseline and to target an LDL cholesterol goal of <70 mg/dL. B
- 10.21 For people with diabetes aged 40–75 years at higher cardiovascular risk, especially those with multiple atherosclerotic cardiovascular disease risk factors and an LDL cholesterol ≥70 mg/dL, it may be reasonable to add ezetimibe or a PCSK9 inhibitor to maximum tolerated statin therapy. C
- 10.22 In adults with diabetes aged >75 years already on statin therapy, it is reasonable to continue statin treatment. B
- 10.23 In adults with diabetes aged >75 years, it may be reasonable to initiate moderate-intensity statin therapy after discussion of potential benefits and risks. C
- 10.24 Statin therapy is contraindicated in pregnancy. B
- 10.25 For people of all ages with diabetes and atherosclerotic cardiovascular disease, high-intensity statin therapy should be added to lifestyle therapy. A
- 10.26 For people with diabetes and atherosclerotic cardiovascular disease, treatment with high-intensity statin therapy is recommended to target an LDL cholesterol reduction of ≥50% from baseline and an LDL cholesterol goal of <55 mg/dL. Addition of ezetimibe or a PCSK9 inhibitor with proven benefit in this population is recommended if this goal is not achieved on maximum tolerated statin therapy. B
- 10.27 For individuals who do not tolerate the intended intensity, the maximum tolerated statin dose should be used. E
- 10.28 For individuals with fasting triglyceride levels ≥500 mg/dL, evaluate for secondary causes of hypertriglyceridemia and consider medical therapy to reduce the risk of pancreatitis. C
- 10.29 In adults with moderate hypertriglyceridemia (fasting or nonfasting triglycerides 175–499 mg/dL), clinicians should address and treat lifestyle factors (obesity and metabolic syndrome), secondary factors (diabetes, chronic liver or kidney disease and/or nephrotic syndrome, hypothyroidism), and medications that raise triglycerides. C
- 10.30 In individuals with atherosclerotic cardiovascular disease or other cardiovascular risk factors on a statin with controlled LDL cholesterol but elevated triglycerides (135–499 mg/dL), the addition of icosapent ethyl can be considered to reduce cardiovascular risk. A
- 10.31 Statin plus fibrate combination therapy has not been shown to improve atherosclerotic cardiovascular disease outcomes and is generally not recommended. A
- 10.32 Statin plus niacin combination therapy has not been shown to provide additional cardiovascular benefit above statin therapy alone, may increase the risk of stroke with additional side effects, and is generally not recommended. A
The more recent STEP trial assigned 8,511 patients aged 60–80 years with hypertension to a systolic blood pressure target of 110 to <130 mmHg (intensive treatment) or a target of 130 to <150 mmHg (34). In this trial, the primary composite outcome of stroke, acute coronary syndrome, acute decompensated heart failure, coronary revascularization, atrial fibrillation, or death from cardiovascular causes was reduced by 26% in the intensive treatment group. In this trial, 18.9% of patients in the intensive treatment arm and 19.4% in the standard treatment arm had a diagnosis of type 2 diabetes. Hypotension occurred more frequently in the intensive treatment group (3.4%) compared with the standard treatment group (2.6%), without significant differences in other adverse events, including dizziness, syncope, or fractures.
The more recent Chronic Hypertension and Pregnancy (CHAP) trial assigned pregnant individuals with mild chronic hypertension to antihypertensive medications to target a blood pressure goal of <140/90 mmHg (active treatment group) or to control treatment, in which antihypertensive therapy was withheld unless severe hypertension (systolic pressure ≥160 mmHg or diastolic pressure ≥105 mmHg) developed (control group) (48). The primary outcome, a composite of preeclampsia with severe features, medically indicated preterm birth at <35 weeks of gestation, placental abruption, or fetal/neonatal death, occurred in 30.2% of female participants in the active treatment group vs. 37.0% in the control group (P < 0.001). The mean systolic blood pressure between randomization and delivery was 129.5 mmHg in the active treatment group and 132.6 mmHg in the control group.
Current evidence supports controlling blood pressure to 110–135/85 mmHg to reduce the risk of accelerated maternal hypertension but also to minimize impairment of fetal growth. During pregnancy, treatment with ACE inhibitors, angiotensin receptor blockers (ARBs), and spironolactone are contraindicated as they may cause fetal damage. Special consideration should be taken for individuals of childbearing potential, and people intending to become pregnant should switch from an ACE inhibitor/ARB or spironolactone to an alternative antihypertensive medication approved during pregnancy. Antihypertensive drugs known to be effective and safe in pregnancy include methyldopa, labetalol, and long-acting nifedipine, while hydralzine may be considered in the acute management of hypertension in pregnancy or severe preeclampsia (49). Diuretics are not recommended for blood pressure control in pregnancy but may be used during late-stage pregnancy if needed for volume control (49,50). The American College of Obstetricians and Gynecologists also recommends that postpartum individuals with gestational hypertension, preeclampsia, and superimposed preeclampsia have their blood pressures observed for 72 h in the hospital and for 7–10 days postpartum. Long-term follow-up is recommended for these individuals as they have increased lifetime cardiovascular risk (51). See Section 15, “Management of Diabetes in Pregnancy,” for additional information.
'내분비내과 > 당뇨병' 카테고리의 다른 글
| 문정동내과, 이전에 인슐린 치료를 받지 않은 제2형 당뇨병에서 Daily Glargine U100와 Weekly Icodec의 비교 (0) | 2023.08.04 |
|---|---|
| 당뇨병 환자에서 고혈압 목표, ADA 2023 (0) | 2023.02.22 |
| 당뇨병에서 혈당 조절 목표 (평균포도당, 당화혈색소, 연속혈당측정), ADA 2023 (0) | 2023.02.12 |
| 제2형당뇨병과 비만/과체중 - 체중 감량, 도움이 되는 약제들 (0) | 2023.02.12 |
| 당뇨병에서 권고되는 예방접종. ADA 2023 (0) | 2023.02.12 |